Share:
Hello all!
This month, let's think about head supports for individuals who use wheelchairs. Essentially, there are 3 circumstances under which we may be considering head supports for individuals – for people who do not have good head control and require head support when seated upright; for people who have good head control when seated upright, but require support of the head when using a tilt or recline feature in seating; and for people who remain seated in a wheelchair in transit and who are required by the transportation provider to have a head support affixed to the wheelchair while the individual is in transit.
As always, when assessing for seating and secondary postural supports, we need to start with the position of the pelvis. The pelvic position influences the position of the head. If you are unsure what I mean by this, slide into a posterior pelvic tilt while sitting. Along with the increased kyphosis in your spine, you either found that your neck was in a forward flexed position while in posterior pelvic tilt, or your neck was extended in order to maintain your forward gaze. Similarly, if you shift into an anterior pelvic tilt, you will again notice that the position of your neck and head changes. This is why before we can begin addressing the position of the head, we must begin with pelvic and trunk positioning.
Once the optimal position of the pelvis and trunk for the individual is found, we can then assess for head support. Just as the placement of our hands on an individual's trunk helps us to assess for a back support for an individual, the placement of our hands on an individual's head helps us to determine the needs for a head support. When we assess for head support placement, we are cognizant of areas on the head that can and cannot take load. Safe areas for positioning include the occipital and sub-occipital areas, the lateral cervical spine, the lateral aspect of the skull superior to the temporal region, and the forehead. Areas to avoid for positioning include the temporal area, the eyes, the mastoid process and the mandible.
Using our hands on an individual's head during the seating assessment will help to determine the optimal head position for the individual, the direction of support required, and the amount of active movement present. All of this information will help to determine the size and types of pad(s) that are required to support the head, the relative placement of the pad(s), the type of hardware required, and its mounting position on the back support. For example, if cervical rotation must be accommodated the direction of force must be aligned between the mounting of the hardware and the pad and the head of the individual. This may mean that an off-set mount is required to move the mount of the head support to one side of the back support to match up the direction of force of the individual's head with the direction of force of the head support.
A generic head support is comprised of the mounting hardware and the various pad choices. This month, we will begin with looking at mounting hardware. There essentially are two different generic types of head support mounts. One type of mount has horizontal and vertical bars, such as the 2 mounts pictured below, to the left. The other style of mount is a gooseneck, as shown in the 2 pictures to the right.
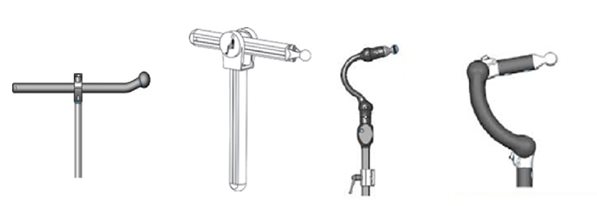
Both types of mounting hardware allow for anterior-posterior adjustment. The benefit of the gooseneck style, in addition to its aesthetic appeal, is that the anterior-posterior adjustment is achieved without a protruding horizontal rod. The protrusion of the horizontal rod can be hazardous to caregiving staff. This is why we often see a tennis ball placed on the end of the horizontal rod to offer some protection for people behind the wheelchair.
Another consideration in selecting mounting hardware is strength and durability. When individuals consistently break the mounting hardware of head supports, perhaps due to tone, the strength of the materials and design must be considered. The image that is second from the left, above, represents a more durable mounting option, as shown by its thicker material. Another option is using a dual mount, wherein two mounts are affixed to the headrest pad and to the back support to provide additional strength.
Typically, a bracket affixes the head support hardware to the back support. Again, there are choices available between regular brackets and flip-back brackets. Some gooseneck style mounting hardware also have a flip-back option built into the neck of the hardware. The benefit of having an available flip back, is that the head support can flip back out of the way for transfers while remaining attached to the wheelchair. Remaining attached to the wheelchair means that the head support is less likely to go missing, and that when the head support is brought upright, it remains in the intended position for the individual. When a head support is repeatedly removed for transfers, there is the possibility that the head support will not be positioned vertically where it was intended.
The difference between having a flip-back option on the gooseneck style mounting hardware versus a flip-back bracket is the height of the lever point. On a flip-back bracket, the whole arm of the mounting hardware and the head support pad are flipped back at a lower pivot point than on a gooseneck style, in which the flip-back mechanism typically is at the base of the gooseneck. This means that the weight and lever arm length are greater and longer when a flip-back bracket is selected than when a gooseneck with a flip-back is selected.
The pad choices for head supports are numerous, and go from very simple single pad systems to multi-pad systems. Next month, we will address pad selection and possible modifications.